The Mechanics of Erection
Erections depend more on blood flow than hormones.
When arousal occurs, the nervous system signals blood vessels in the penis to dilate.
This dilation depends on nitric oxide (NO), produced by the endothelium, the single-cell
layer lining all blood vessels. Nitric oxide relaxes smooth muscle in arterial walls,
allowing blood to rush in and create the hydraulic pressure that produces an erection.
Know your vascular age
Take the free calculator. 15 questions. Your estimated vascular age score in minutes.
Take the Free Calculator →
Testosterone plays a role. It influences libido, arousal, and the baseline tissue
environment. But testosterone cannot produce an erection without adequate blood flow.
A man with optimal testosterone but impaired vascular function will still struggle.
The Erection Pathway
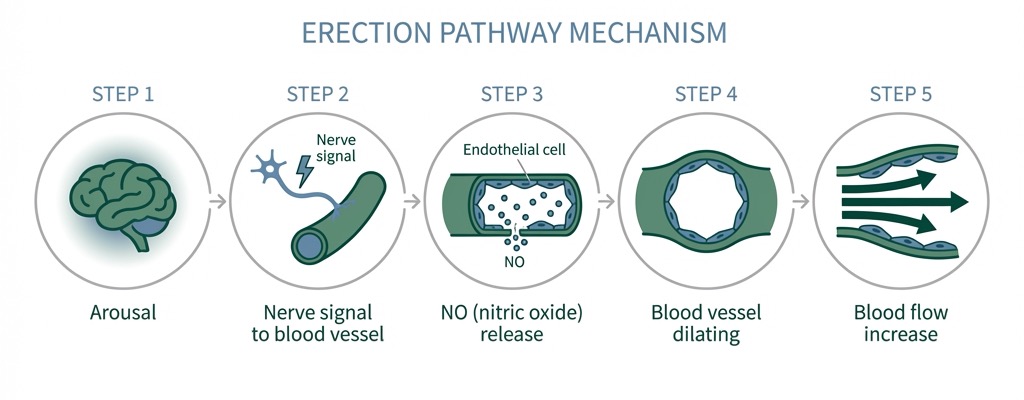
The process begins with arousal, which triggers a neural signal. This signal prompts
endothelial cells to release nitric oxide. The nitric oxide causes vascular smooth muscle
to relax, allowing arteries to dilate. Blood flows in, and the hydraulic pressure produces
an erection.
The limiting factor is often somewhere in this pathway, most commonly reduced nitric oxide
production due to endothelial dysfunction.
The Hormone Approach
The hormone approach to ED assumes the problem is insufficient testosterone. Treatment
typically involves testosterone replacement therapy (TRT), which increases circulating
testosterone levels through injections, gels, or pellets.
This can work when testosterone is genuinely low and is the limiting factor. If a man's
testosterone is well below normal range, libido may be reduced and erections may suffer
as a downstream effect.
However, TRT does not address the vascular mechanics of erection. If the endothelium
is damaged and nitric oxide production is impaired, higher testosterone won't solve
the blood flow problem. The additional testosterone hits a bottleneck: the vessels
can't deliver what the tissues need.
The Vascular Approach
The vascular approach asks: is the delivery system working?
If endothelial function is impaired, if nitric oxide production is reduced or the
glycocalyx (the protective lining of blood vessels)
is degraded, blood flow to all organs is affected. This includes the brain (contributing
to brain fog), muscles (contributing to fatigue), and the penis (contributing to ED).
ED, brain fog, and fatigue often appear together
because they share a common mechanism: impaired blood flow.
Comparing the Two Approaches
| Factor |
Hormone Approach |
Vascular Approach |
| Root assumption |
Testosterone is the limiting factor |
Blood flow is the limiting factor |
| What it addresses |
Hormone levels |
Endothelial function, NO production |
| Testing focus |
Total/free testosterone, SHBG |
ADMA, ApoB, homocysteine, CRP |
| Treatment duration |
Typically lifelong |
Finite protocol with maintenance |
| Other benefits |
May improve mood, muscle, energy |
May improve cognition, energy, cardiovascular health |
| Dependency created |
Yes (suppresses natural production) |
No (supports natural function) |
How Do You Know Which Applies?
Signs of hormone-driven ED:
- Libido is significantly reduced (not just erection quality)
- Morning erections have disappeared entirely
- Testosterone testing shows levels below normal range
- No other symptoms suggesting vascular involvement
- No response to vasodilator medications
Signs of vascular-driven ED:
- Erection quality declined gradually over years
- Libido is present but erections don't follow
- Brain fog, fatigue, or cold extremities accompany ED
- Vasodilator medications (Viagra, Cialis) work well
- Testosterone levels are normal or borderline
- Labs look "normal" but you don't feel right
- Risk factors present: metabolic syndrome, hypertension, insulin resistance
The Overlooked Connection
Here's what's often missed: ED is frequently a vascular early warning sign.
The penile arteries are among the smallest in the body. When endothelial dysfunction
develops, these small vessels are affected first, often years before larger vessels
show problems. ED can appear 3-5 years before a cardiovascular event.
Treating ED with pills or hormones without investigating the vascular component
may mean missing an important signal about systemic health. The symptom gets managed;
the underlying condition continues to progress.
The GRN Vascular Protocol
The GRN Protocol focuses on supporting
vascular function through targeted biomarker assessment and a continuously adaptive protocol. We test biomarkers that indicate
endothelial health, markers your regular doctor
likely doesn't check, and target the underlying vascular architecture.
This doesn't replace hormones or medication. It addresses a different layer of
the problem: the delivery system. For many men, improving vascular function improves
erectile function without additional intervention.
Can Both Be True?
Yes. Some men have both low testosterone and impaired vascular function.
The question is which to address first. If you add testosterone to a compromised
vascular system, you may see limited improvement, and you've committed to lifelong
hormone replacement. If you address vascular function first, you may find that
hormones normalize on their own, or that the hormone replacement you eventually
choose works better because the delivery system is now functional.
The vascular-first approach doesn't reject
hormones. It suggests investigating the delivery system before adding more fuel.